

بررسی نتایج پاتولوژی حاصل از وکیوم بیوپسی (VABB) میکروکلسیفیکاسیون¬های مشکوک پستان تحت گاید ماموگرافی و بررسی فراوانی موارد بدخیم آن در سال 98-99 در انستیتو کانسر بیمارستان امام خمینی
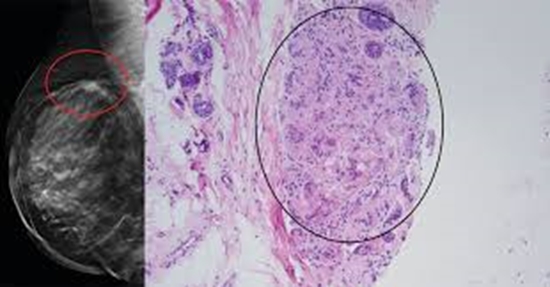
Objective: Breast microcalcification is examined by mammographic diagnosis based on morphology and diffusion. While most microcalcification seen on mammography are benign, microcalcification can be the first evidence of breast cancer. The aim of this study was to evaluate the pathological results of vacuum biopsy of suspected breast microcalcification under the direction of mammography and to evaluate the frequency of malignancies.
Methods: In cross-sectional study, 256 microcalcification suspected of malignancy were examined under vacuum biopsy during 1398 and 1399 in Imam Khomeini Hospital. Prior to biopsy, all patients were evaluated and classified according to BIRADS, and the morphology of microcalcification and their distribution in breast tissue were evaluated. Clinical information, history and cases of microcalcification upgrade in 6-month follow-up in patients with atypical or benign pathology were also determined.
Results: Suspected breast microcalcification were with BIRADS 4b (81.3%), BIRADS 4c (17.3%) and BIRADS 5 (0.8%). Benign lesions were seen in 179 patients (69.9%) and malignant lesions in 77 patients (30.1%). Fibrocystic changes were the most common benign lesion (36.1%) and DCIS was the most common malignant lesion (76.5%). Breast composition were 126 (49.2%) grade c and 82 (32%) grade b, respectively. The association between malignancy and BIRADS was significant (P<0.0001). The highest frequency of malignancy was seen in BIRADS 4c and BIRADS 5 microcalcification (77.3% and 100%, respectively). The most common subtype of microcalcification were amorphous punctate (41.5%), fine pleomorphic (29.4%) and the most common distribution of microcalcification were multiple group (59%) and single group (17.8%), respectively. The prevalence of malignancy was higher in fine pleomorphic (63.8%) and fine linear branching (100%) microcalcification. The relationship between microcalcification morphology and malignancy was not significant (P = 0.723). The relationship between microcalcification malignancy and age, family history of cancer, personal history of cancer, breast composition was not significant (P<0.05 in all). In 11 patients with atypical pathology, the pathology result of 2 patients (18.2%) was DCIS after surgery and 9 patients (81.8%) were stable under 6-month follow-up. In microcalcifications with suspicious appearance BIRADS4, sensitivity, specificity, positive predictive value and negative diagnostic value were determined to be 48.6%, 94.51%, 77.27% and 82.69%, respectively.
Conclusion: Microcalcifications are rarely malignant and invasive. Due to the high prevalence of DCIS malignancy, a biopsy vacuum can be used to detect morphological microcalcification and suspected diffusion for early detection of breast cancer. The malignancy in atypical patients during the 6-month follow-up period, which led to high-risk pathology, emphasizes the importance of monitoring and imaging in these patients.


ارسال نظر